DEFINITIONS AND NORMAL VALUES
Arterial blood pressure is defined as the lateral pres sure exerted by the column of blood on wall of arteries. The pressure is exerted when blood flows through the arteries Generally, the term blood pressure refers to arterial blood pressure.
Arterial blood pressure is expressed in four terms
1.Systolic blood pressure 2.Diastolic blood pressure. 3. Pulse pressure. 4.Mean arterial blood pressure.
SYSTOLIC BLOOD PRESSURE Systolic blood pressure (systolic pressure) is defined as the maximum pressure exerted in the arteries during systole of heart
Normal systolic pressure:
120 mm Hg (110 to 140 mm Hg)
DIASTOLIC BLOOD PRESSURE
Diastolic blood pressure (diastolic pressure) is defined as the minimum pressure exerted in the arteries during diastole of heart
Normal diastolic pressure:
80 mm Hg (60 to 80 mm Hg)
PULSE PRESSURE
Pulse pressure is the difference between the systolic pressure and diastolic pressure
Normal pulse pressure:
40 mm Hg (120 - 80 = 40)
MEAN ARTERIAL BLOOD PRESSURE
Mean arterial blood pressure is the average pressure existing in the arteries. It is not the arithmetic mean of systolic and diastolic pressures. It is the diastolic pressure plus one third of pulse pressure. To determine the mean pressure, diastolic pressure is considered than the systolic pressure. It is because the diastolic period of cardiac cycle is longer (0.53 second) than the systolic period (0.27 second)
Normal mean arterial pressure:
93 mm Hg (80+ 13 = 93).
Formula to calculate mean arterial blood pressure Mean arterial blood pressure
=Diastolic pressure 1/3 of pulse pressure
= 80 +40 3 = 93.3 mm Hg
VARIATIONS
Blood pressure is altered in physiological and pathological conditions Systolic pressure is subjected for variations easily and quickly and its variation occurs in a wider range. Diastolic pressure is not subjected for easy and quick variations and its variation occurs in a narrow range.
PHYSIOLOGICAL VARIATIONS
1. Age
Arterial blood pressure increases as age advances. Table 100.1 shows systolic and diastolic pressures at different age.
2. Sex
In females, up to the period of menopause, arterial pressure is 5 mm Hg, less than in males of same age. After menopause, the pressure in females becomes equal to that in males of same age.
3. Body Built
Pressure is more in obese persons than in lean persons.
4. Diurnal Variation
In early morning, the pressure is slightly low. It gradually increases and reaches the maximum at noon. It becomes low in evening.
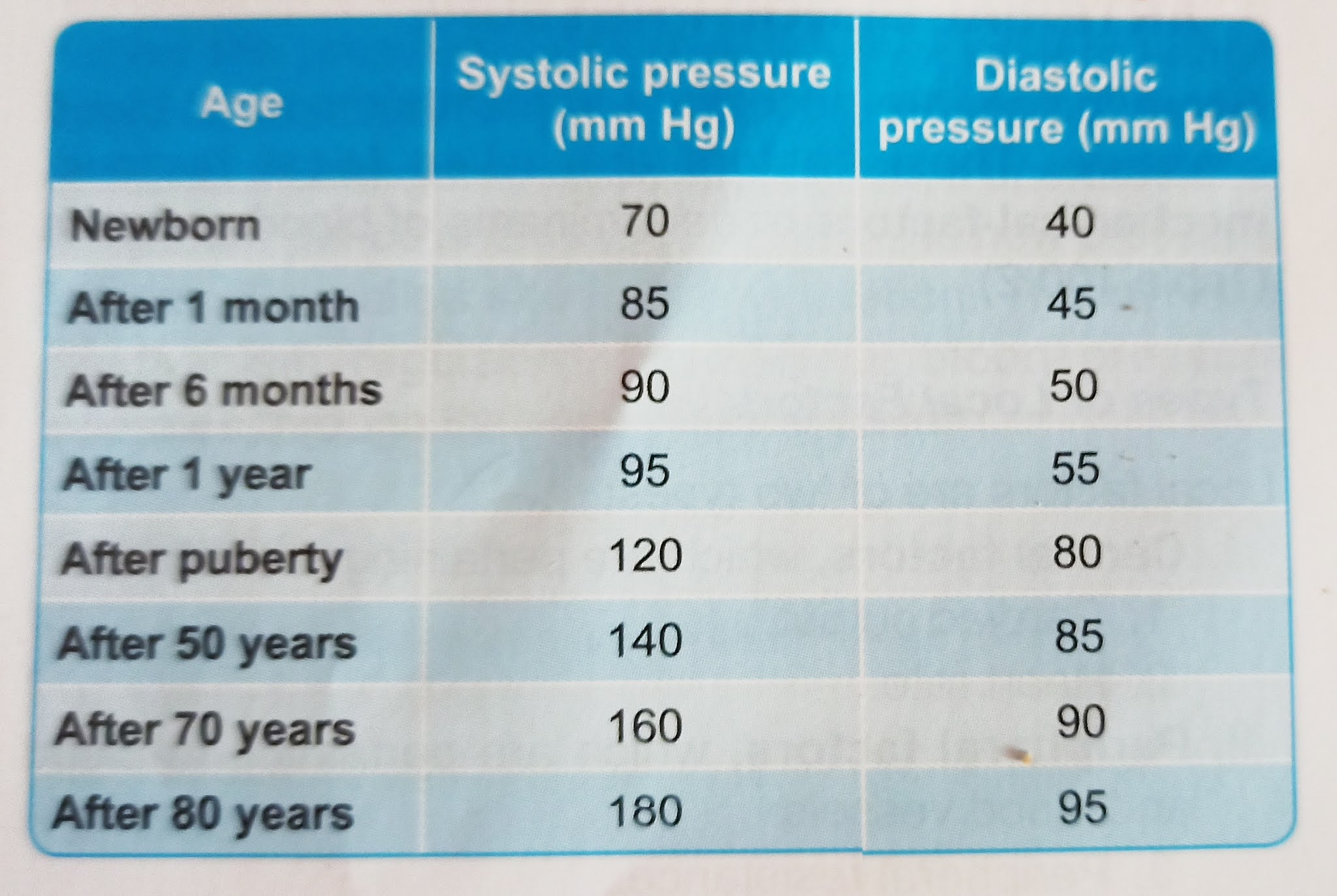 |
| Arterial blood pressure in different age |
5. After Meals
Arterial blood pressure is increased for few hours after meals due to increase in cardiac output.
6. During Sleep
Usually, the pressure is reduced up to 15 to 20 mm Hg during deep sleep. However, it increases slightly during sleep associated with dreams
7. Emotional Conditions
During excitement or anxiety, the blood pressure is increased due to release of adrenaline
8. After Exercise
After moderate exercise, systolic pressure increases by 20 to 30 mm Hg above the basal level due to increase in rate and force of contraction and stroke volume Normally, diastolic pressure is not affected by moderate exercise. It is because, the diastolic pressure depends upon peripheral resistance, which is not altered by moderate exercise.
After severe muscular exercise, systolic pressure rises by 40 to 50 mm Hg above the basal level. But the diastolic pressure reduces because the peripheral resistance decreases in severe muscular exercise. More details are given in Chapter 114
PATHOLOGICAL VARIATIONS
Pathological variations of arterial blood pressure are hypertension and hypotension. Refer applied physiology of this chapter for details.
DETERMINANTS OF ARTERIAL BLOOD PRESSURE: FACTORS MAINTAINING ARTERIAL BLOOD PRESSURE:
Some factors are necessary to maintain normal blood pressure. These factors are called local factors, mechanical factors or determinants of blood pressure .
Types of Local Factors
Local factors are of two types: 1. Central factors, which are pertaining to the heart
1. Cardiac output. 2. Heart rate.
II. Peripheral factors, which are pertaining to blood and blood vessels:
3. Peripheral resistance. 4. Blood volume 5. Venous return.
6. Elasticity of blood vessels.
7. Velocity of blood flow. 8. Diameter of blood vessels.
9. Viscosity of blood.
CENTRAL FACTORS
1. Cardiac Output
Cardiac output is the important factor which maintains systolic blood pressure. Systolic pressure is directly proportional to cardiac output. Whenever the cardiac output increases, the systolic pressure is increased and when cardiac output is less, the systolic pressure is reduc Cardiac output increases in muscular exercise, emotional conditions, etc. So, in these conditions, the systolic pressure is increased. In conditions like myocardial infarction, the cardiac output decreases, resulting in fall in systolic pressure.
2. Heart Rate
Moderate changes in heart rate do not affect arterial blood pressure much. However, marked alteration in the heart rate affects the blood pressure by altering cardiac output.
PERIPHERAL FACTORS
3. Peripheral Resistance
Peripheral resistance is the important factor, which maintains diastolic pressure. Diastolic pressure is directly proportional to peripheral resistance Peripheral resistance is the resistance offered to the blood flow at the periphery. Resistance is offered at arterioles, which are called the resistant vessels. When peripheral resistance increases, diastolic pressure is increased and when peripheral resistance decreases, the diastolic pressure is decreased.
 |
| Local factor determining arterial blood pressure. |
4. Blood Volume
Blood pressure is directly proportional to blood volume. Blood volume maintains the blood pressure through the venous return and cardiac output. If the blood volume increases, there is an increase in venous return and cardiac output, resulting in elevation of blood pressure.
5. Venous Return
Blood pressure is directly proportional to venous return. When venous return increases, there is an in crease in ventricular filling and cardiac output, resulting in elevation of arterial blood pressure.
6. Elasticity of Blood Vessels
Blood pressure is inversely proportional to the elasticity of blood vessels. Due to elastic property, the blood vessels are distensible and are able to maintain the pressure. When the elastic property is lost, the blood vessels become rigid (arteriosclerosis) and pressure increases as in old age. Deposition of cholesterol, fatty acids and calcium ions produce rigidity of blood vessels and atherosclerosis, leading to increased blood pressure.
7. Velocity of Blood Flow
Pressure in a blood vessel is directly proportional to the velocity of blood flow. If the velocity of blood flow increases, the resistance is increased.
 |
| Effect of blood volume and venous return on arterial blood pressure. |
8. Diameter of Blood Vessels
Arterial blood pressure is inversely proportional to the diameter of blood vessel. If the diameter decreases, the peripheral resistance increases, leading to increase in the pressure.
9. Viscosity of Blood
Arterial blood pressure is directly proportional to the viscosity of blood. When viscosity of blood increases, the frictional resistance is increased and this increases the pressure.
REGULATION OF ARTERIAL BLOOD PRESSURE
Arterial blood pressure varies even under physiological conditions. However, immediately it is brought back to normal level because of the presence of well-organized regulatory mechanisms in the body. Body has four such regulatory mechanisms to maintain the blood pressure within normal limits:
I. Nervous mechanism or short-term regulatory mech anism. II. Renal mechanism or long-term regulatory mechanism.
III. Hormonal mechanism.
IV. Local mechanism.




























